The Nobel Foundation’s Remarkable Oversight: The Salk Polio Vaccine
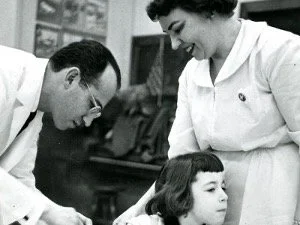
Jonas Salk inoculating a participant in the trial of the polio vaccine.
First published June 7, 2026
The threat of poliomyelitis (polio) in the summer months was an overwhelming concern of parents when those of us over 70 were children. The development of a vaccine to prevent polio was a profoundly impactful addition to preventive medicine. Yet, the Nobel Committee refused to honor this singular benefit to human health.
Alfred Nobel’s third and final will that established the five prizes stipulated that they should be awarded “…to those who, during the preceding year, shall have conferred the greatest benefit on mankind”. The Nobel Foundation, wisely, has ignored the stipulation that the achievement be in the prior year. Jonas Salk, however, met Nobel’s criterion for the Prize in Physiology or Medicine in every respect. First, it was an achievement of enormous and enduring benefit to humankind; and, second, if Salk had been selected for the Prize in 1956, it would have been for his seminal accomplishment the year before, when the results of his very large clinical trial of the inactivated poliovirus vaccine showed its beneficial effect.
On April 12, 1955, it was announced that the Salk vaccine was safe and effective in a massive trial of 1.8 million children. It was approved for use by the U.S. government the same day. In May 1955, my future father-in-law, an internist in Buffalo, NY, obtained polio vaccine and flew to Boston and from there drove to Wellesley, Massachusetts, to inoculate his younger daughter Alice Jo (my future wife) and her older sister, Joan, both students at Wellesley College. This was an example of the urgency and significance of this development. He did not wait the month for the end of the school year and their return home for summer. The prevention of polio is one of the great achievements of vaccinology. Few, if any, Prizes would have met so closely Nobel’s explicit directions.
In 1954, John Enders, Thomas Weller and Frederick Robbins in Boston shared the Nobel Prize in Physiology or Medicine for enabling the cultivation of poliovirus in non-nervous tissue, which technique later allowed the development of attenuated, live vaccines for polio and other viral diseases. Using this technique, Albert Sabin and his colleagues working in Cincinnati successfully field-tested the attenuated, live, oral poliovirus vaccine. It was licensed in the United States in 1962.
Why did Salk neither win nor share the Prize with Sabin a few years later? Fifty years after a Prize has been awarded, the Nobel Foundation opens its records to their deliberations. A description of the reasoning surrounding the selection of the scientists who shared the Prize in 1954 and the failure to recognize Salk in 1955 or 1956 has been published. A key virologist in the deliberations considered that the work of Enders’ team had “… a revolutionary effect on the discipline of virology”. He described Salk’s work as a technical achievement, not prize-worthy. This conclusion came despite its prevention of a profoundly disabling human disease. I wonder if Alfred Nobel would have agreed. After all, the complexity of the science need not be a prerequisite of its benefit to humankind, Nobel’s primary expectation. The Nobel Foundation consultant’s opinion carried the day, “not Salk”. In addition, both the Boston and Cincinnati groups thought Salk’s killed vaccine an inferior approach to an attenuated live-viral vaccine. In theory, that may have been correct but not in practice in all situations. Their disagreements on approach were public and pointed.
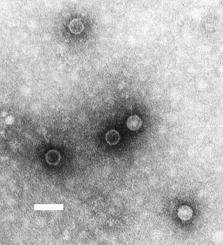
Electron microscopy of several poliovirus particles.
Today, the Salk virus-inactivated vaccine is the preferred approach to preventing polio in the United States. The oral live-attenuated vaccine has been used for mass immunization in developing countries with higher risks of polio outbreaks because it is easy to administer (liquid drops), inexpensive, and provides intestinal immunity to stop community fecal-oral spread of the virus. This spread of the attenuated virus is beneficial as it magnifies the effect of the vaccine. In effect, the population spread of the attenuated virus results in widespread immunity more rapidly. However, a restoration of virulence may occur in an inoculated individual or in someone who obtained the attenuated live virus by fecal-oral spread from an inoculated individual. This rare event, the ability to revert and cause paralytic polio, occurs in, on average, one of 1.5 million vaccinated persons. Today, in Societies in which polio is uncommon with a highly immunized population, the virus-inactivated (Salk) vaccine is considered safest. Thus, in the United States, only the inactivated (Salk) vaccine has been approved for use since 2000.
It is ironic that Salk was deemed undeserving of the Nobel Prize, whereas in 1955 and thereafter, the Salk vaccine prevented innumerable cases of paralytic polio and today, over 70 years later, the Salk vaccine is the safest approach for the prevention of polio in developed countries.
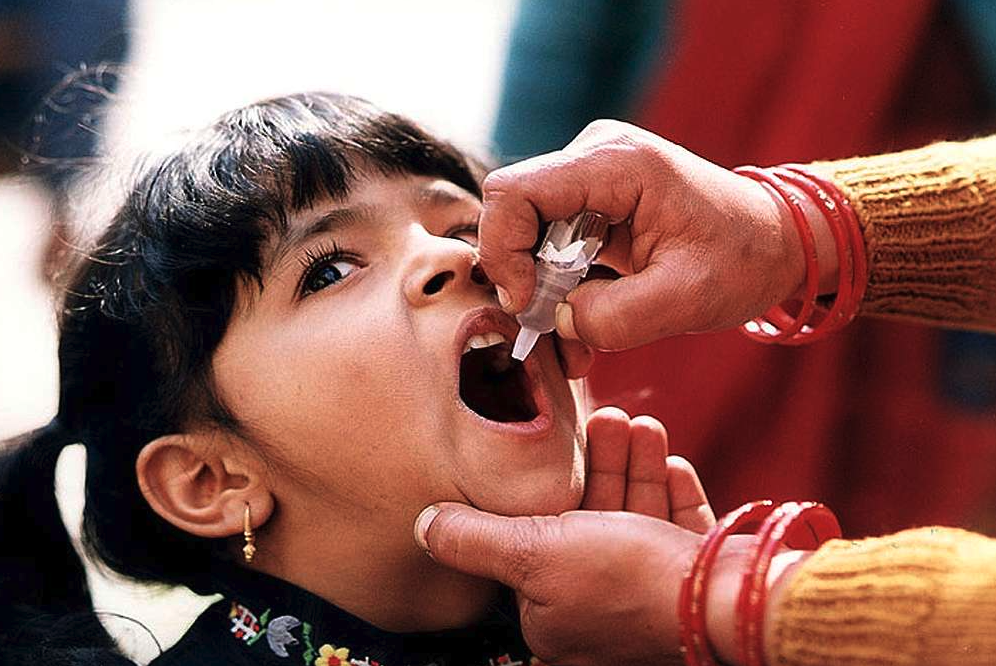
A young Indian girl receiving a dose of oral polio vaccine by a trained healthcare worker.
An important underpinning of Salk’s work was the establishment of the National Foundation for Infantile Paralysis, nicknamed The March of Dimes, by Franklin D. Roosevelt in 1937. Roosevelt contracted paralytic polio as an adult and lost all use of both legs. The country, especially mothers, rallied around this fundraising effort to find a medical solution to the disease. The centerpiece was the installation of cardboard dime holders where shoppers could insert a dime or two in stores and other public sites around the country. A dime in 1938 is worth well over two dollars in 2026. This funding was vital to underwriting Salk’s development of the vaccine and provision of care for the afflicted.

Iron lungs supporting polio victims with respiratory muscle paralysis.
The president of the organization was Basil O’Connor, a former law partner of Franklin Roosevelt. He served in this role for over 30 years. He built an extensive network of chapters throughout the U.S., and their fundraising and research grants program was instrumental in the development of the vaccine. The amount of money devoted to Salk’s vaccine research was 7.5 million dollars in the early 1950’s, which would equate to over 95 million dollars in 2026. The March of Dimes also covered medical bills and treatment costs, ensuring that no patient went without care due to an inability to pay from 1938, just after its inception, to the 1950s and the availability of the vaccine. Patient-care dollars translated into billions of dollars in today’s monetary value. The Foundation purchased and transported thousands of iron lungs to hospitals across the country to help paralyzed patients breathe. They helped fund long-term care facilities and physical therapy to rehabilitate patients affected by the disease. Their financial contribution to the care of polio patients and the eventual prevention of the disease by vaccination was singular. It was an early example of the enlistment of the general public in the solution of a disabling and life-altering health problem.